 Close
Close

There are approximately 7 million people living with heart and circulatory diseases in the UK. With an ageing population and improved survival rates, this number is likely to rise still further. Heart and circulatory diseases cause a quarter of all deaths in the UK; an average of 420 people each day[1].
At the Institute of Nuclear Medicine we perform a variety of non-invasive cardiovascular imaging studies:
Myocardial perfusion imaging (nuclear stress tests) for the detection and management of coronary artery disease using SPECT and PET. Stress modalities include vasodilator pharmacologic and dobutamine stress testing.
Cardiac CT angiography.
- Viability studies to assess for the extent of myocardial infarction.
- Radionuclide cineangiograms (MUGA studies) to evaluate heart function.
What do we offer?
We are one of a few centres in the U.K which carry out cardiac PET imaging as well as SPECT imaging. PET has the advantage of improved resolution and advances in hardware have improved its diagnostic capability. Uniquely, PET allows quantification, which can help detect global abnormalities which may be missed by qualitative SPECT scans such as in the case of balanced ischaemia.
Information obtained from SPECT/PET scans can be used to:
- identify blockages in the coronary arteries
- determine whether someone has had a heart attack
- try to predict those at high risk for a heart attack
- assess a patient’s condition after bypass surgery or angioplasty
We are also one of the few centres in the UK that offers a “one stop shop ability” to perform cardiac PET/SPECT imaging assessing myocardial function alongside same day cardiac CT angiography which can map the anatomical abnormality to the area of abnormal perfusion.
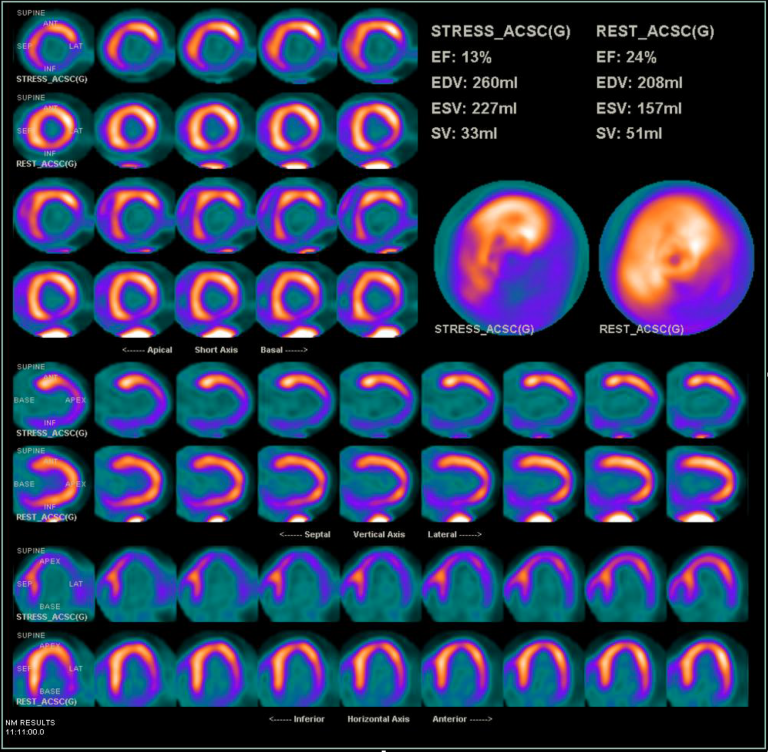
Myocardial perfusion PET study showing partly reversible reduced tracer uptake in the inferior lateral segments.
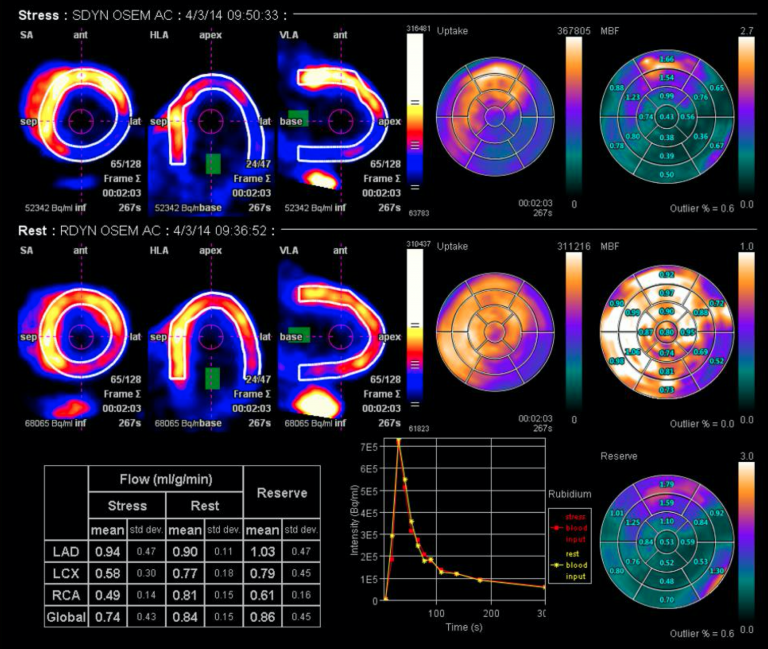
Quantification confirming reduced flow to the inferior (RCA) territory in the same patient.
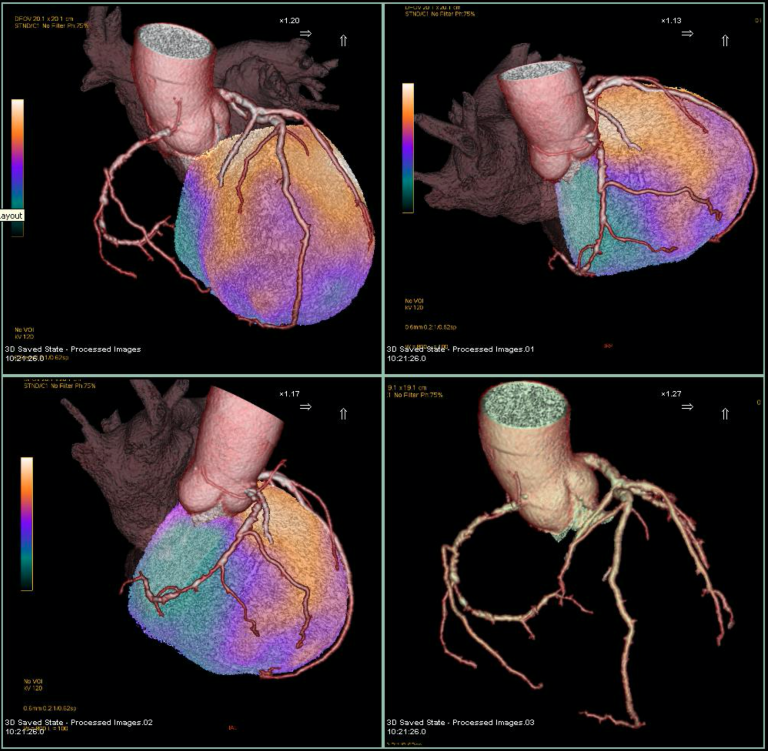
Perfusion data obtained from the cardiac PET study fused with the coronary CT from the same patient, demonstrating the area of myocardium involved (in purple).
Amyloid imaging
Cardiac amyloidosis is an important cause of restrictive cardiomyopathy and congestive heart failure. Its variable clinical symptoms, nonspecific ECG and echocardiographic findings means cardiac amyloidosis can be a diagnostic challenge and is usually underdiagnosed.
Uptake of Tc-99m MDP correlates with biopsy-proven cardiac amyloidosis and Tc-99m MDP imaging can be used as a noninvasive tool in the differential diagnosis of cardiac amyloid.
Sarcoid imaging
Cardiac involvement is associated with a poorer prognosis in patients with sarcoidosis. Growing data supports the role of 18F-fluorodeoxyglucose (18F-FDG) PET in the diagnosis and risk stratification of patients with cardiac sarcoidosis.
18F-FDG PET has high diagnostic accuracy and has been shown to be equally or more sensitive than delayed enhancement CMR in detecting myocardial lesions from cardiac sarcoidosis*
Practically, it and can be used in patients in whom CMR is contraindicated e.g. impaired renal function and/or those with implanted metallic devices. 18F-FDG PET also allows assessment of disease activity, assessment of perfusion pattern and has the advantage of evaluating the extent of extra cardiac systemic disease and allows evaluation in response to treatment.
Our group published work on the role of FDG PET CT in Diagnostic accuracy and prognostic value of simultaneous hybrid 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging in cardiac sarcoidosis [2]
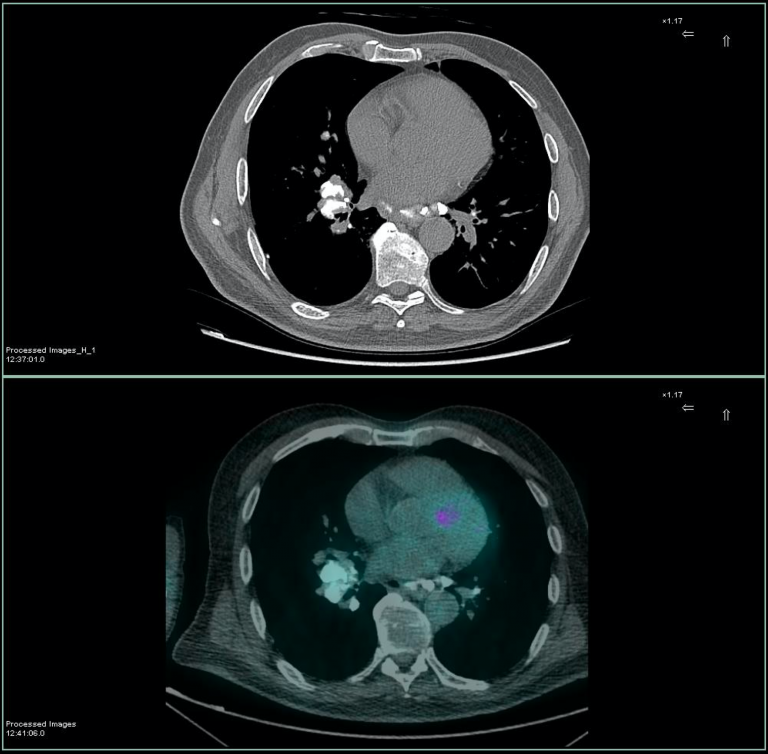
Axial CT and fused FDG PET CT showing patchy myocardial uptake in a patient with known sarcoidosis (calcified mediastinal lymphadenopathy also present). The patient was confirmed to have biopsy proven myocardial sarcoidosis.
Research
Non-invasive virtual histological assessment of the left ventricle would have a number of clinical diagnostic and therapeutic applications. Some current techniques e.g. CMR ‘scar’ imaging using Late Gadolinium Enhanced images, parametric mapping and Cardiac Diffusion Tensor Imaging (cDTI). All these techniques, however, use intravenous contrast. The ability if textural Analysis, a post processing imaging technique to differentiate between the myocardial structural changes in Hypertrophic Cardiomyopathy (HCM) Aortic Stenosis (AS) and Cardiac Amyloid in Cardiac Magnetic Resonance Imaging (CMR) was assessed by our group.
Content by Dr Deena Neriman
References
1. British Heart Foundation. Factsheet November 2018.
2. Diagnostic accuracy and prognostic value of simultaneous hybrid 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging in cardiac sarcoidosis. Eleanor C. Wicks, Leon J. Menezes, Anna Barnes, Saidi A. Mohiddin, Neha Sekhri, Joanna C. Porter, Helen L. Booth, Emily Garrett, Riyaz S. Patel, Menelaos Pavlou, Ashley M. Groves, and Perry M. Elliott.