 Close
Close

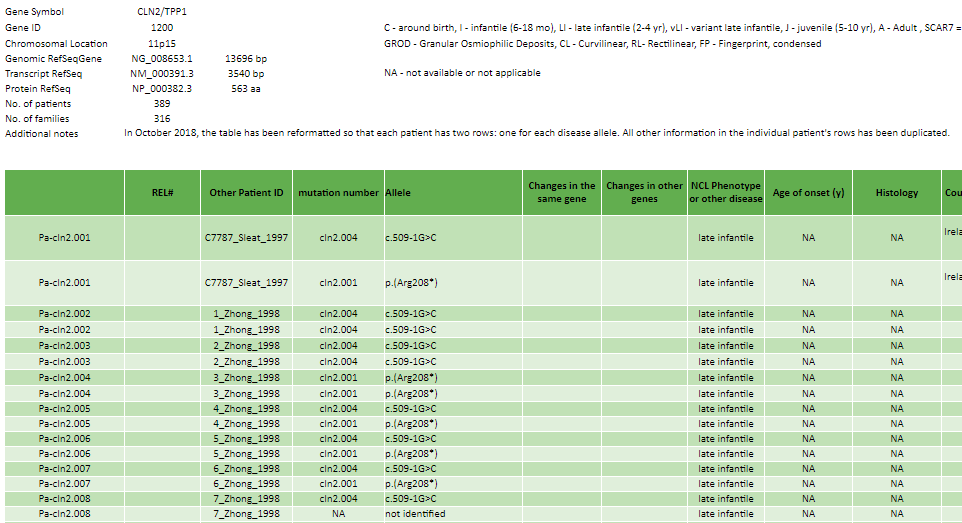
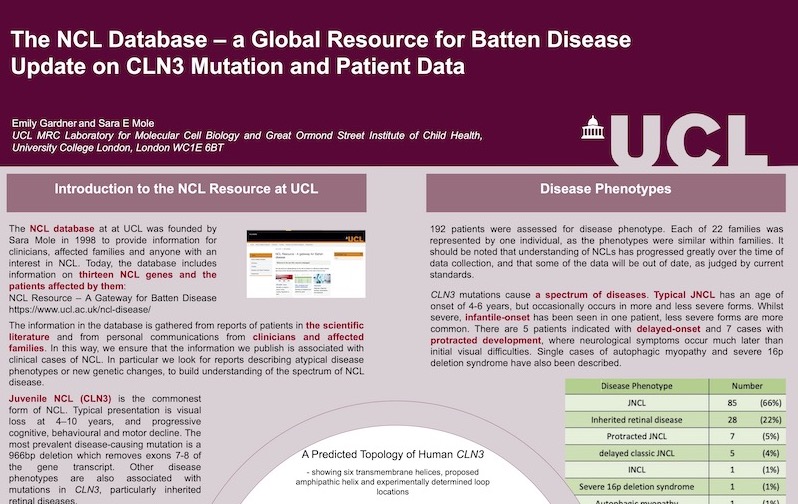
NCL Resource - A gateway for Batten disease
This site serves as a global gateway for any with an interest in or affected by Batten disease, also known as the neuronal ceroid lipofuscinoses (NCL), or who wish to find out more.





One user reported in Nov 2009 "After scouring the internet for the past few weeks and sifting through scientific journals, personal testimonies, and clinical studies, I continue to return to your NCL website. At least for me, it is by far the most accessible, user-friendly, and informative site for the layperson that I have found and subsequently used. Thank you for providing this resource--to the global community, indeed", and another more briefly in 2012 "I thought your Batten webpage was fantastic".
Website maintained by Emily Gardner and Sara Mole, University College London
This page uodated October 2023