 Close
Close

The British Regional Heart Study (BRHS) was established to examine the factors responsible for heart disease and stroke in Great Britain.
Origins & Background of the British Regional Heart Study (1975-78):
The origins of the British Regional Heart Study (BRHS) lie in the Seven Countries Study of Ancel Keys and his colleagues, in the Framingham Study in the United States and in the work in the United Kingdom of Professor J N Morris and his collaborators in the MRC Social Medicine Unit.
Professor Gerry Shaper and colleagues submitted a 5-year proposal to the Medical Research Council to examine the factors responsible for the considerable regional variation in coronary heart disease, hypertension, and stroke in Great Britain, and to determine the causes of these conditions in order to provide a rational basis for recommendations towards their prevention. This proposal embraced the water hardness hypothesis but extended the potential of the data collected to produce a more substantial and wider ranging enquiry into the causes of CHD both at the individual and the regional level.
Baseline BRHS data (1978-80):
In 1978-80, a longitudinal study of cardiovascular disease was initiated in 7735 men aged 40-59 years drawn from one general practice in each of 24 British towns – this comprised the baseline sample of the BRHS cohort. The towns were selected using data from a previous study of 253 towns (S J Pocock, A G Shaper et al. British Regional Heart Study: geographic variations in cardiovascular mortality, and the role of water quality Br Med J. 1980 May 24; 280(6226): 1243–1249). A wide range of physical, physiological, biochemical and haematological measurements were made in these men and questionnaires relating to their lifestyle and medical and family histories were completed.
Follow up of the BRHS cohort
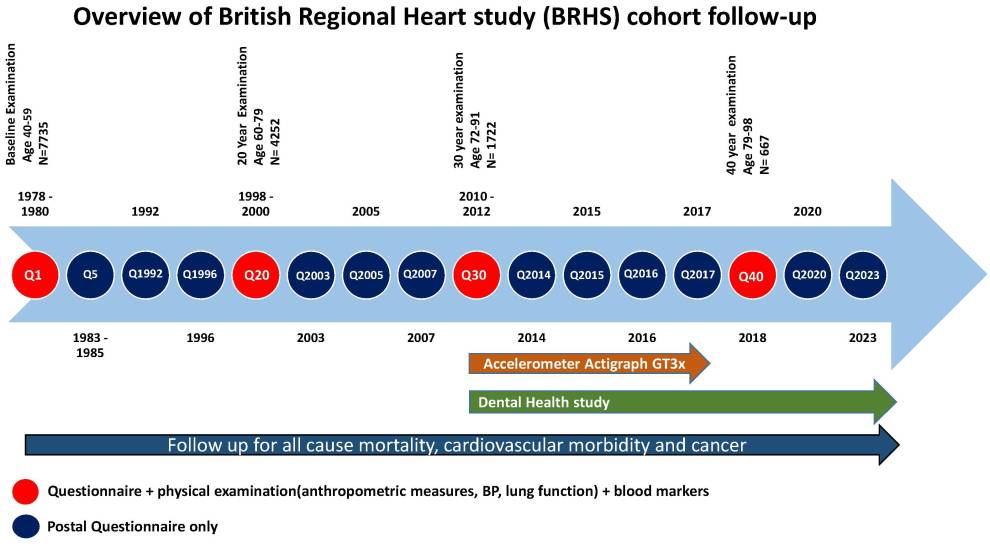
The prospective follow up of the BRHS has produced information relating to almost every aspect of coronary heart disease, hypertension and stroke in middle-aged and older men in Great Britain and has extended its enquiries and analyses to diabetes mellitus and to cancer. The figure below shows an overview of the BRHS cohort follow-up.
The longitudinal follow-up of all the BRHS participants has allowed investigating the incidence of mortality and morbidity relating to cardiovascular disease and to other conditions such as diabetes mellitus and cancer, with reference to the interplay between individual and environmental risk factors. Follow-up has been achieved through close collaboration with the general practices, the participants and central registers (for example, the Office of Population and Census Surveys (OPCS), Health and Social Care Information Centre (HSCIC), NHS Digital). The prospective study contains reports of major cardiovascular events among study participants made by general practitioners obtained from regular (two-yearly) review of the General Practice (GP) records (including all hospital and clinic correspondence) and participant completed postal questionnaires. The cohort participants have also been followed-up through regular physical examinations and postal questionnaires - see figure below.
Follow up through physical examinations:
The cohort has been followed up by at regular intervals for re-examinations at ages 60–79 years (1998–2000) and 71–92 years (2010–12) and 78-98 years (2018-19). At each time point, clinical measurements were carried out on each man by a team of specially trained nurses. The re-examinations were carried out in the original 24 towns where men were recruited at baseline. Participants who had migrated from their original town were offered a choice between examination either in their original town, another BRHS town of their choice or examination in London.
| Physical examination Year | Follow-up time point | Age range | Number of participants examined | Response rate % |
|---|---|---|---|---|
1978-1980 | Baseline | 40-59 | 7735 | 78 |
1998-2000 | 20-year follow-up | 60-79 | 4252 | 77 |
2010-2012 | 30-year follow-up | 71-92 | 1722 | 55 |
2018-2019 | 40-year follow-up | 78-98 | 667 | 41 |
Through the physical re-examinations, the cohort was followed-up on a wide range of physical, physiological, biochemical and haematological measurements (see figure below).
Figure: British Regional Heart Study (BRHS) follow-up time line (Kimble R et al. IJE 2022,1–8. https://doi.org/10.1093/ije/dyac122)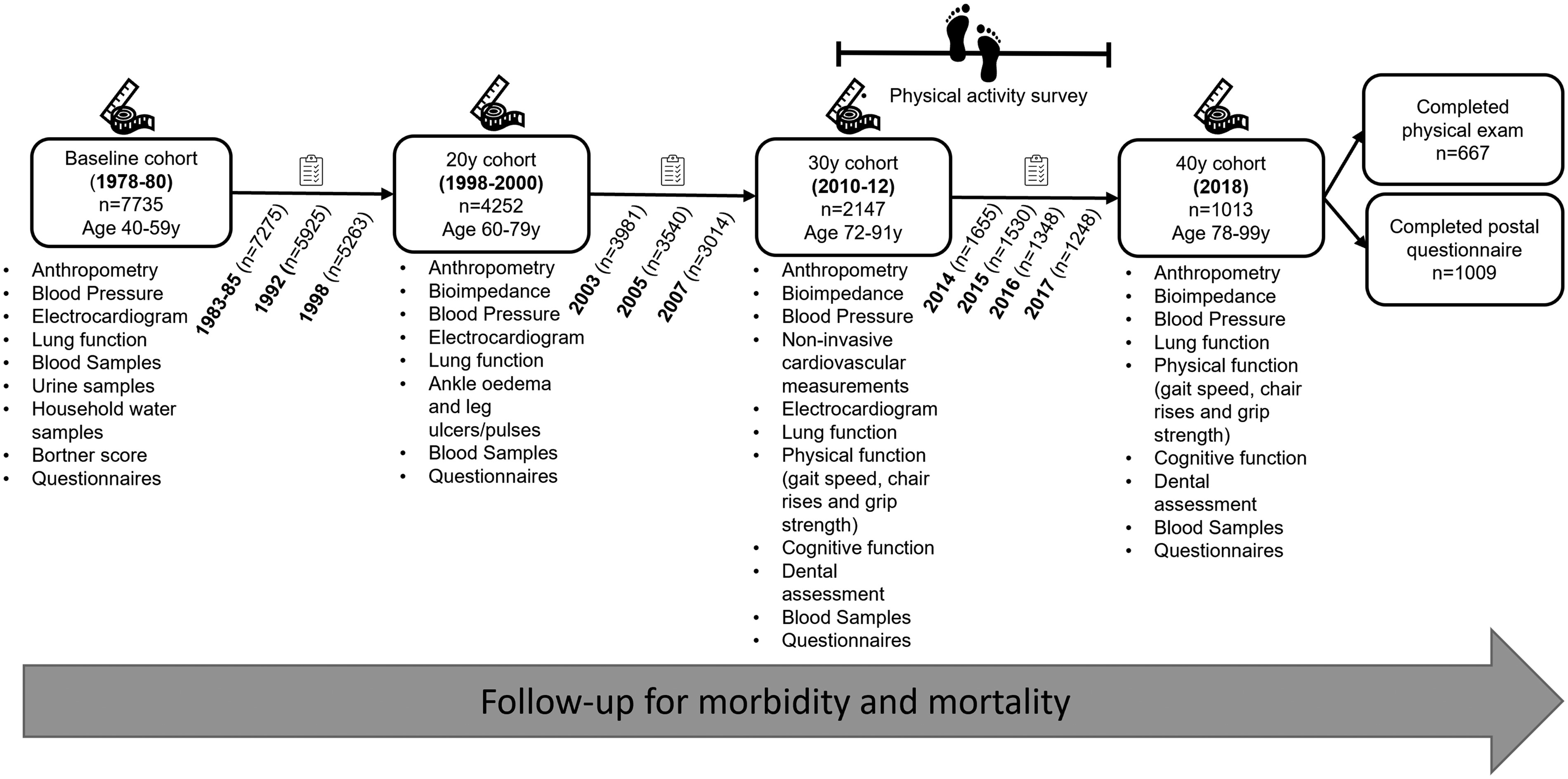
A general overview of the physical measurements and biomarkers at each physical examination can be found by visiting the links below:
- Overview of measurements collected through physical examinations 1978 – 2018
- Overview of biomarkers at physical examination time point 1978 – 2018
Further data documentation and data dictionaries at each physical examination time point can be found in: Explore BRHS data by time point.
Follow up through postal questionnaires:
The BRHS cohort has been followed up through periodic postal questionnaires collecting detailed information on a wide range of health-related behaviours, overall health, diagnoses and self-reported symptoms and social factors. These questionnaires are a valuable resource for research into the health status of older adults in the 21st century- see Table 1 below for questionnaire, timepoint, age range and response.
A general overview of the topics covered in these questionnaires and the questions included at each study time point is available by visiting the link below.
Further data documentation and data dictionaries and copies for each questionnaire can be found in explore BRHS data by time point.
Table 1: Questionnaire follow-up: timepoint, age range and response rates
| Questionnaire Year | Study Timepoint | BRHS study time point (year of follow-up) | Age range of cohort | Number of completed questionnaires | Response rate % |
|---|---|---|---|---|---|
1978-80 | Baseline (Q1) | Baseline | 40-59 | 7735 | 78 |
1983-85 | Q5 | 3-5 year | 45-64 | 7275 | 98 |
1992 | Q1992 | 12-14 year | 52-74 | 5925 | 91 |
1996 | Q1996 | 16-18 year | 56-78 | 5263 | 88 |
1998-2000 | Q20 - Main | 20 year (Main questionnaire) | 60-79 | 4252 | 77 |
1998-2000 | Q20 - Physical Activity & Diet | 20 year (Physical Activity & Diet Qr) | 60-79 | 4582 | 83 |
2003 | Q2003 | 23-25 year | 62-85 | 3981 | 80 |
2005 | Q2005 | 25-27 year | 64-87 | 3540 | 79 |
2007 | Q2007 | 27-29 year | 66-89 | 3014 | 75 |
2010-2012 | Q30 | 30 year | 71-92 | 2137 | 68 |
2014 | Q2014 | 34-36 year | 73-96 | 1655 | 64 |
2015 | Q2015 | 35-37 year | 74-97 | 1530 | 66 |
2016 | Q2016 | 36-38 year | 75-98 | 1348 | 65 |
2017 | Q2017 | 37-39 year | 76-99 | 1248 | 66 |
2018 | Q2018 | 40 year | 78-98 | 1009 | 62 |
2020 | Q2020 | 42-44 year | 80-100 | 803 | 62 |
Follow up for morbidity through General Practice (GP) records
The GP record review is a review of BRHS participants’ GP records (i.e. primary care records) for specified non-fatal events mostly related to cardiovascular disease, although this has subsequently been extended to include additional cardiovascular events and treatment, diabetes, cancer, dementia and frailty (Table 2). The aim of the GP record review has been to identify and record the date of these events. The reviews have been carried out since baseline (1978-80) through to 2022 at intervals, typically every one or two years. More detailed information and data documentation of the GP record review can be found in GP record review in explore BRHS data by time point.
Table 2: Morbidity events collected through General Practice (GP) records
| Event type | Year when data collection for events commenced |
|---|---|
Myocardial infarction (MI) | Baseline (1978) |
Angina | Baseline (1978) |
Stroke | Baseline (1978) |
Transient ischemic attack (TIA) | Baseline (1978) |
Coronary artery bypass graft (CABG) | 1983 |
Percutaneous transluminal coronary angioplasty, (PTCA) | 1983 |
Diabetes | 1988 |
Heart failure (HF) | 1996 |
Cancer | 1996 |
Peripheral vascular disease (PVD) | 1998 |
Deep vein thrombosis (DVT) | 2000 |
Pulmonary embolism (PE) | 2000 |
Abdominal aortic aneurysm | 2000 |
Atrial fibrillation | 2014 |
Dementia | 2014 |
COVID-19 | 2020 |
Frailty/Frailty score | 2020 |
Follow up for mortality
All BRHS cohort participants (n=7735) have been flagged for death notifications through Central Registries in England and Scotland since the study baseline (1978-80). Information is received on the date of death, and coded cause of death - International Classifications of Disease codes (ICD9, ICD10). This data is provided annually by NHS Digital or its predecessor organisations. More detailed information and data documentation of follow-up mortality can be found in follow-up mortality in explore BRHS data by time point
Follow up for cancer
All BRHS cohort participants have been flagged for cancer notification through the Cancer Registry since baseline (1978-80). Information is received on the date of cancer diagnosis, the site and type of cancer. The type of cancer is provided in the form of an International Classifications of Disease code (ICD9, ICD10). This data is provided by NHS Digital or its predecessor. More detailed information and data documentation of follow-up cancer events can be found in follow-up Cancer events in explore BRHS data by time point
Follow up through linkage to routine health records
In 2018, the BRHS cohort was linked to routine health records - NHS Hospital Episode Statistics (HES), Mental Health Services Data Set (MHSDS) and Diagnostic Imaging Datasets (DID). This linkage provides retrospective and prospective data.
- Hospital Episode Statistics (HES) is a database containing details of all admissions, A&E attendances and outpatient appointments at NHS hospitals in England.
- Mental Health Services Data Set (MHSDS) collects data from the health records of individuals who are in contact with mental health services- our study remit is dementia focused.
- The Diagnostic Imaging Dataset (DID) is a central collection of detailed information about diagnostic imaging tests carried out on NHS patients, The DID captures information about the details of the test (type of test and body site).
Spin-off studies
The BRHS extended its observations to younger men and women and to children drawn from schools in 10 of the same 24 towns (Ten Town Study). The studies in children led by Professor Peter Whincup (St George's, University of London) have been particularly productive and have been extended to other towns in Great Britain.
A parallel cohort of women The British Women's Heart and Health Study (BWHHS), was set up in 1999 to investigate the risk factors, causes, prevention and use of health services for cardiovascular disease, in women.